|
Overview
Leg length difference (LLD) is primarily when the hips are not level, causing a limp from side to side. Most practitioners divide LLD into anatomical or functional. Anatomical is when there is a true difference in the length of the tibia/fibula or the femur bone, or both. While functional LLD are either the shortening or lengthening of a limb, secondary to joint contracture or muscle imbalances.  Causes Some limb-length differences are caused by actual anatomic differences from one side to the other (referred to as structural causes). The femur is longer (or shorter) or the cartilage between the femur and tibia is thicker (or thinner) on one side. There could be actual deformities in one femur or hip joint contributing to leg length differences from side to side. Even a small structural difference can amount to significant changes in the anatomy of the limb. A past history of leg fracture, developmental hip dysplasia, slipped capital femoral epiphysis (SCFE), short neck of the femur, or coxa vara can also lead to placement of the femoral head in the hip socket that is offset. The end-result can be a limb-length difference and early degenerative arthritis of the hip. Symptoms In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity. Diagnosis The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used. Non Surgical Treatment The key to treatment of LLD in a child is to predict what the discrepancy is at maturity. If it is predicted to be less than 2 cm., no treatment is needed. Limb length discrepancies of up to 2 or 2.5 cm. can be compensated very well with a lift in the shoe. Beyond 2.5 cm., it becomes increasingly difficult to compensate with a left in the insole. Building up the shoe becomes uncosmetic and cumbersome, and some other way of compensating for the discrepancy becomes necessary. The treatment of LLD is long-term treatment, and involves the physician and patient?s family working together as a team. The family needs to weigh the various options available. If leg lengthening is decided on, the family needs to understand the commitment necessary to see it through. The treatment takes 6 months to a year for completion, and complications can happen. But when it works, the results are gratifying.  how do you get taller in a day? Surgical Treatment Surgery to shorten the longer leg. This is less involved than lengthening the shorter leg. Shortening may be done in one of two ways. Closing the growth plate of the long leg 2-3 years before growth ends (around age 11-13), letting the short leg catch up. This procedure is called an epiphysiodesis. Taking some bone from the longer leg once growth is complete to even out leg lengths. Surgery to lengthen the shorter leg. This surgery is more involved than surgery to shorten a leg. During this surgery, cuts are made in the leg bone. An external metal frame and bar are attached to the leg bone. This frame and bar slowly pull on the leg bone, lengthening it. The frame and bar must be worn constantly for months to years. When the frame and bar are removed, a leg cast is required for several months. This surgery requires careful and continued follow-up with the surgeon to be sure that healing is going well.
0 Comments
Overview
 A bunion is a bony lump on the side of your foot, which develops when your big toe starts to angle towards your second toe. The bunion will eventually cause you discomfort and pain. The skin over the lump can become red, blistered or infected. A fluid-filled space called a bursa may also develop under your skin in this area and this can be painful if it becomes inflamed. This is called bursitis. The deformity of your big toe combined with a bunion is sometimes referred to as hallux valgus. Causes Essentially, bunions are caused by a disruption of the normal interworking of the bones, muscles, ligaments and tendons that comprise your feet, often from wearing shoes that squeeze the toes or place too much weight-bearing stress on them. However, it should be pointed out that other causes or factors in the development of bunions can include flat feet or low arches in the feet, some forms of arthritis, problems with foot mechanics, foot injuries and neuromuscular disorders such as cerebral palsy. Arthritis in the MTP joint, for example, can degrade the cartilage that protects it, and other problems may cause ligaments to become loose. Pronation, walking in a way that your foot rolls inwards, increases your risk for developing bunions. SymptomsThe major symptom of bunions is a hard bump on the outside edge of the foot or at the base of the big toe. Redness, pain and swelling surrounding or at the MTP joint can also occur. Diagnosis People with bunions may be concerned about the changing appearance of their feet, but it is usually the pain caused by the condition that leads them to consult their doctor. The doctor will evaluate any symptoms experienced and examine the affected foot for joint enlargement, tissue swelling and/or tenderness. They will also assess any risk factors for the condition and will ask about family history. An x-ray of the foot is usually recommended so that the alignment of big toe joint can be assessed. This would also allow any other conditions that may be affecting the joint, such as arthritis, to be seen. Non Surgical Treatment Because they are bone deformities, bunions do not resolve by themselves. The goal for bunion treatment is twofold: first, to relieve the pressure and pain caused by irritations, and second to stop any progressive growth of the enlargement. Commonly used methods for reducing pressure and pain caused by bunions include the use of protective padding, often made from felt material, to eliminate the friction against shoes and help alleviate inflammation and skin problems. Removal of corns and calluses on the foot. Changing to carefully fitted footwear designed to accommodate the bunion and not contribute toward its growth. Orthotic devices, both over-the-counter and custom made-to help stabilize the joint and place the foot in the correct position for walking and standing. Exercises to maintain joint mobility and prevent stiffness or arthritis. Splints for nighttime wear to help the toes and joint align properly. This is often recommended for adolescents with bunions, because their bone development may still be adaptable. 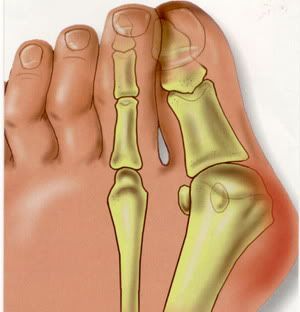 Surgical Treatment Bunion surgery is most often a day case or one night in hospital. Surgery can be done under ankle block (patient awake) or general anaesthetic. It is best to rest with the foot elevated for the first 2 weeks after surgery. The foot is bandaged and a special sandal supplied by the hospital is worn for 6 weeks. Sensible shoes are to be worn for a further 6 weeks after the bandages are removed. It will take between 3-6 months for the swelling to go down. It will take 12 months before everything completely settles. It is also important to remember that not all bunion operations are entirely successful. Overview
 A bunion, also known as hallux valgus, is a painful deformity that develops at the base of the big toe. Bunions are caused when the big toe pushes and bends inward towards the other toes. This displaces the bones of the joint, causing it to protrude in a way that looks like a large growth. Bunions develop due to a variety of factors. Some people inherit feet that are more susceptible due to their shape and structure, having flat feet for instance. But bunions can be made worse by the wrong shoe, or by carrying extra weight or prolonged periods of standing or walking. Causes Bunions are most often caused by an inherited faulty mechanical structure of the foot. It is not the bunion itself that is inherited, but certain foot types that make a person prone to developing a bunion. Although wearing shoes that crowd the toes won?t actually cause bunions, it sometimes makes the deformity get progressively worse. Symptoms may therefore appear sooner. SymptomsA bony bump along the edge of the foot, at the base of the big toe (adjacent to the ball of the foot) Redness and some swelling at or near the big toe joint. Deep dull pain in the big toe joint. Dull achy pain in the big toe joint after walking or a sharp pain while walking. The big toe is overlapping the second toe, resulting in redness, calluses, or other irritations such as corns. Diagnosis Diagnosis begins with a careful history and physical examination by your doctor. This will usually include a discussion about shoe wear and the importance of shoes in the development and treatment of the condition. X-rays will probably be suggested. This allows your doctor to measure several important angles made by the bones of the feet to help determine the appropriate treatment. Non Surgical Treatment Podiatrists will treat bunions conservatively, using paddings and orthotics, which are devices that are made to protect the joint or deviate pressure away from it. Sometimes bunions will develop overlying callus or corns. These can be removed by a podiatrist, but if the area is irritated again by wearing ill-fitting footwear, the corn will grow back. Most people with this condition have flat feet, so arch supports are often recommended.  Surgical Treatment Bunion surgery is most often performed as an out-patient, this means you go home that same day. It will likely be done at a hospital or out-patient (ambulatory) surgery center. The anesthetic choices with bunion surgery are local with sedation, spinal or general anesthesia. You wouldn?t expect that a small bunion would be treated exactly the same as a large one. Over the years, surgeons have developed dozens of methods to surgically correct bunions. But don?t worry because only a handful of methods are used today. With most bunion surgeries today, the procedure involves a combination of soft-tissue rebalancing of ligaments and tendons as well as bone work to re-align the foot structure. You may have heard people say they had their ?bunion shaved.? In most cases, the surgery often involves much more than simply shaving the bunion. The shaving part of the procedure is called an ?exostectomy? and often performed in conjunction with other methods. Overview
 The common bunion is a localized area of enlargement of the inner portion of the joint at the base of the big toe. The enlargement actually represents a misalignment of the big toe joint (metatarsal phalangeal joint) and, in some cases, additional bone formation. The misalignment causes the big toe to point outward (medically termed hallux valgus deformity) toward the smaller toes. This deformity is progressive and will increase with time. The enlarged joint at the base of the big toe (the first metatarsophalangeal joint, or MTP joint) can become inflamed with redness, tenderness, and pain. A small fluid-filled sac (bursa) adjacent to the joint can also become inflamed (bursitis), leading to additional swelling, redness, and pain. A more deep joint pain may occur as localized arthritis develops in later stages of the deformity. A less common bunion is located at the joint at the base of the smallest (fifth) toe. This bunion is sometimes referred to as a tailor's bunion or bunionette. Causes Long periods of pressure from a tight-fitting shoe can cause the inflammation and the pain. This often happens when the big toe is forced into a position where it presses inward and overlaps the second toe. The base of the big toe then is pushed beyond normal alignment of the foot, resulting in the prominence typical of a bunion. SymptomsThe main sign of a bunion is the big toe pointing towards the other toes on the same foot, which may force the foot bone attached to it (the first metatarsal) to stick outwards. Other symptoms may include a swollen, bony bump on the outside edge of your foot, pain and swelling over your big toe joint that's made worse by pressure from wearing shoes, hard, callused and red skin caused by your big toe and second toe overlapping, sore skin over the top of the bunion, changes to the shape of your foot, making it difficult to find shoes that fit. These symptoms can sometimes get worse if the bunion is left untreated, so it's best to see a GP. They'll ask you about your symptoms and examine your foot. In some cases, an X-ray may be recommended to assess the severity of your bunion. Anyone can develop a bunion, but they're more common in women than men. This may be because of the style of footwear that women wear. Diagnosis Your doctor can identify a bunion by examining your foot. Watching your big toe as you move it up and down will help your doctor determine if your range of motion is limited. Your doctor will also look for redness or swelling. After the physical exam, an X-ray of your foot can help your doctor identify the cause of the bunion and rate its severity. Non Surgical Treatment Treatment options are based on the severity of the deformity and symptoms. Nonsurgical treatments usually are enough to relieve the pain and pressure on the big toe. Your doctor may tell you to start wearing roomy, comfortable shoes and use toe padding or a special corrective device that slips into your shoes to push the big toe back into its proper position. To help relieve pain, you can take over-the-counter medications such as acetaminophen (Tylenol) or ibuprofen (Advil, Motrin and others). Whirlpool baths also may help to ease discomfort.  Surgical Treatment If your bunion has progressed to the point where you have difficulty walking, or experience pain despite accommodating shoes, you may need surgery. Bunion surgery realigns bone, ligaments, tendons and nerves so your big toe can be brought back to its correct position. Orthopedic surgeons have several techniques to ease your pain. Many bunion surgeries are done on a same-day basis, requiring no hospital stay, using an ankle-block anesthesia. A long recovery is common and may include persistent swelling and stiffness. |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
July 2017
Categories |
 RSS Feed
RSS Feed
